OK. I read Balko’s hit pieces. Here, here, here (and a side comment attempt at minimizing this article, here, which failed). They were criticisms of Coleman Hughes for supporting this video:
We can summarize Balko’s analysis as this:
1. Balko and his buddy willemedia claim that the Maximal Restraint Technique (MRT) was taught as a temporary hold to be used only long enough for police officers to administer a restraint device called a hobble. This is incorrect. The MRT is the use of the restraining device itself. A prior search of older versions of the policy manual will show they actually had two devices capable of being used for the MRT, the hobble and the Wrap. The Wrap was discontinued. It is for this reason that there is a variable that paraphrased, says, a. if a hobble is used… with no b. The reason for this is not because there is an option where the person is not hobbled in the MRT, but because option b. is the wrap. In that situation there were two options, the side recovery position or sitting the person up. But the Wrap was discontinued, and option b. was deleted. Balko follows the same error as the Fall of Minneapolis (TFOM) (and Chauvin’s attorney, if I recall) in claiming that prone restraint with the knee was MRT. Balko even makes this claim later, that they are different, but does not realize this actually invalidates his own arguments, not the majority of those made by the documentary he calls TFOM.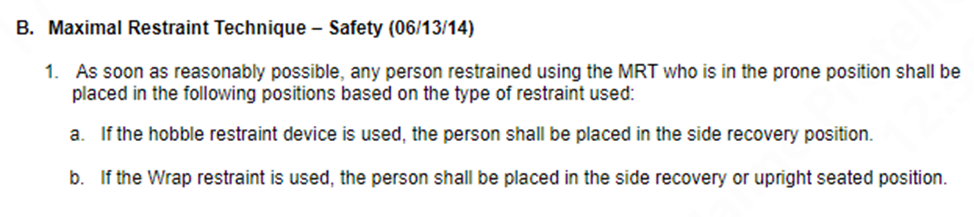
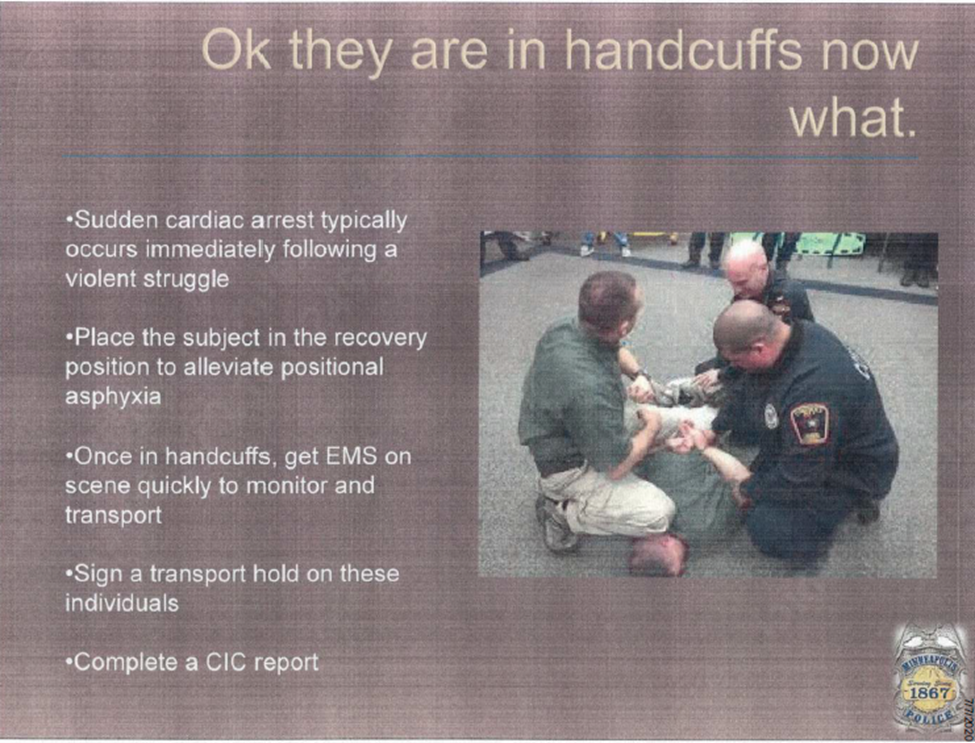
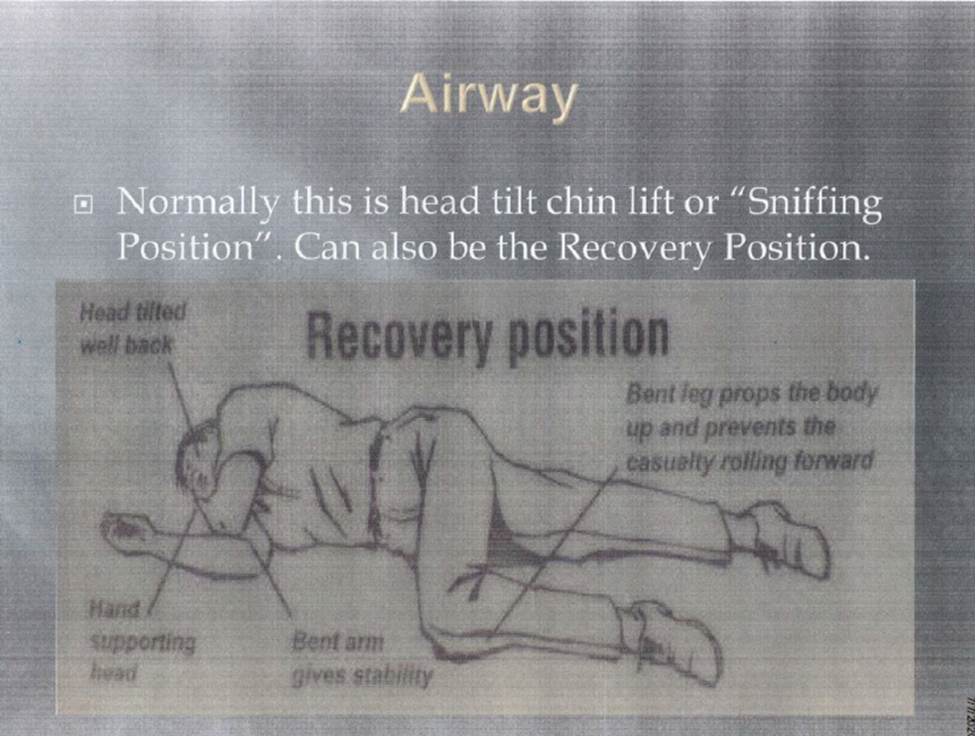
2. MPD policy manual’s discussion of MRT states that it “shall only be used in situations where handcuffed subjects are combative and still pose a threat to themselves, officers or others, or could cause significant damage to property if not properly restrained.” This is correct, but this does not apply to the prone restraint used by Chauvin. Nor is MRT mentioned on the slide that mentions the recovery position that many falsely claim is MRT. Handcuffs are not hobbles, nor MRT because the detainee is in a prone position. Key point, no hobble device is shown on the slide, and that is further evidence, that it is not MRT that is being discussed. MRT can be eventually performed from the prone restraining position, but the prone restraining position is not MRT. Nor does the recovery position show hobbles either.2. MPD policy manual’s discussion of MRT states that it “shall only be used in situations where handcuffed subjects are combative and still pose a threat to themselves, officers or others, or could cause significant damage to property if not properly restrained.” This is correct, but this does not apply to the prone restraint used by Chauvin. Nor is MRT mentioned on the slide that mentions the recovery position that many falsely claim is MRT. Handcuffs are not hobbles, nor MRT because the detainee is in a prone position. Key point, no hobble device is shown on the slide, and that is further evidence, that it is not MRT that is being discussed. MRT can be eventually performed from the prone restraining position, but the prone restraining position is not MRT. Nor does the recovery position show hobbles either.
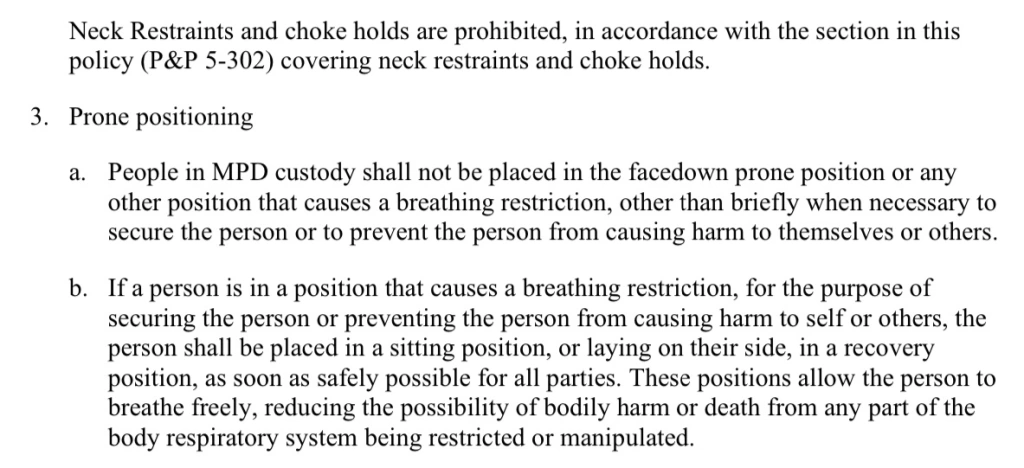
3. Balko further points to the portion of the manual instructing police to roll suspects into a recovery position “as soon as reasonably possible” when they have been placed in the MRT technique. But as Balko well knows, and he would reference later, the prone restraint position is not MRT. They considered doing MRT but didn’t end up using the technique. so, this analysis fails. Even if MRT had been done, this analysis still fails, I will explain later.
4. Floyd was not visibly struggling against Chauvin once he was taken to the ground. This is provably false as he was still struggling while on the ground and kicked Officer Lane. It is one of the reasons they considered MRT. They eveintually found the hobble but decided not to apply it because the fire truck was supposedly imminent.
5. Chauvin allegedly ignored all of Floyd’s pleas that he couldn’t breathe. Not true. If he had, he wouldn’t have called the EMT. His reaction may have been less urgent because most of those pleas started when he was not on the ground and trying to stop them from putting him in the squad car. Furthermore, it was Floyd who requested to be put on the ground. It is those, either false cries, or possibly drug induced inability to breathe ones, which could have been why Chauvin did not take Floyd’s cries on the floor as critical evidence of breathing distress.
5. Chauvin’s response of “Then stop talking, stop yelling. It takes heck of a lot of oxygen to talk.” As proof of callousness, is then negated by Balko himself, when he states: “Chauvin’s comment echoes a common retort from officers when a suspect pleads that he is unable to breathe — “If you can talk, you can breathe.” This is incorrect.” Balko doesn’t realize that he just provided evidence that this is a common misconception among police and thus an honestly held belief that if you can talk you can breathe. Reasonableness of belief.
6. Balko mentions that Lane suggested putting Chauvin on his side. Again, we have determined that MRT did not occur. But Lane suggests the possibility of excited delirium, so further analysis is required. What is Chauvin’s response? That he has called the EMT. Key point, the fire station was only blocks away. In fact, one of the witnesses mentions this. The fire truck ends up going to the wrong address, and the ambulance ends up arriving first, even though the fire station was much closer. As far as Chauvin knew, the EMT would be arriving at any moment, so it was reasonable to stay put. Especially if they had not found the hobble to put Floyd in the MRT. Remember, the fear mentioned wasn’t positional asphyxia, but excited delirium, which is a risk to both the officers, and to the person being arrested.
5. Smith v Minneapolis. In 2010, a man named David Smith died under similar circumstances. Smith died while lying face-down with an MPD officer’s knee in his back. Like Chauvin, the officer continued to put his weight on Smith even after Smith became unresponsive. Smith’s family settled their lawsuit against the city for $3 million. Part of the settlement was a requirement that MPD provide better training on positional asphyxia and the importance of rolling suspects into a recovery position as soon as possible. While this is true, there is no actual evidence that any extensive training was given to all officers. In fact, an investigation by the Minneapolis Police Conduct Oversight Commission (MPCOC) found scant evidence that positional asphyxia was trained on at all, and that all the focus was on excited delirium. If positional asphyxia was barely trained on, at the individual level, what chance do you think it was trained at the group level? As Balko himself stated, he beleived most medical experts beleived that, at various points over nine-and-a-half minutes, Chauvin and the other officers had multiple knees and elbows pushing down on Floyd’s back, wedged into his ribs, and jammed into the back of his neck. All of that pressure coming from multiple directions collapsing Floyd’s diaphragm into the hard pavement. The handcuffs then further restricted his ability to move into a position that would allow him to expand his chest and ribs. The claim isn’t that Chauvin’s knee killed Floyd, but that the collective pressure of three cops killed Floyd. The evidenc that is missing is on group training on positional asphyxia were each individual might not cause it, but collectivley they could. This does suggest a guilty party, the Minneapolis Police Department, but not Chauvin. In fact, the motive Chauvin and company were thrown under the bus by the upper echelon of the MPD may have been to avert focus on this fact.
https://www.mprnews.org/story/2020/07/28/mpd-records-suggest-scarce-training-on-dangers-of-improper-restraints
6. Balko makes much ado about the slide photo where the prone restraint position using a knee is seen, not MRT where the officer is shifting his weight backward, and most of his weight is on his heel, and makes a comparison with the photo of Chauvin that was used at trial where he is more upright, and none of his weight is resting on his foot. A few problems with this analysis. One, this slide, as Balko himself has noted was new and was only seen by Lane. So what weight distribution was seen on an image would not apply to Chauvin. Furthermore, that is a frozen moment in time, and we do not know how this would look dynamically. All we know is that it clearly depicts a prone restraining position with a knee near the neck such as the one Chauvin used. Which is evidence that the technique was not an anomaly in the department. Another key point. Chauvin had used this technique before, and we know this because prior complaints had been filed and those cases were reviewed. More importantly, Chauvin was not reprimanded because his technique passed muster. For armchair hindsight people to claim he was supposed to know Floyd would be at risk of dying, when he used the same technique successfully and without health incident before, and which the department reviewed and green lighted, is asinine.
7. MPD officials testified at the trial that officers were taught that the MRT requires “light to moderate pressure.” This claim is repeated in the video that Balko touts. There are a few problems with this. One. As we said before Chauvin never applied MRT. Two, the manuals say nothing about applying light to moderate pressure while executing the MRT. What the manuals say is that when applying the neck restraint (chokehold) there are two techniques, the conscious restraint and the unconscious restraint. The conscious restraint requires light to moderate pressure when compressing the neck, and the unconscious neck restraint requires as much pressure as is adequate to render the person unconscious. Key points, reviewing, the prior manuals, we can easily determine that neck restraints specifically apply to blood chokes, where the officer wraps his arm around the detainee’s neck and pressures the carotid arteries on both sides of the neck. The leg was added in the last iteration, more than likely because officers were taught to triangle choke using their legs from the ground. What would be instructional is to see the combatives instructional manual used by police. No one has ever referenced this. What is clear though, is that it is not referencing a knee on shoulder and neck restraining technique that cannot focus on compressing the carotid arteries. No matter what the idiot claiming to do MMA claimed that it was a blood choke. You need to pressure both carotids for a blood choke, or as the police calls it, a neck restraint, for it to work. A slight or moderate squeeze will make you woozy, and if you squeeze harder, it will render you unconscious. Furthermore, in the fantastical scenario where a knee on shoulder and neck could qualify as a neck restraint (it doesn’t), the manual literally says that unconscious neck restraints are allowed when a subject is exhibiting active resistance in order to gain control of the subject; and if lesser attempts at control have been or would likely be ineffective. Considering the long struggle the officers had with Floyd, such use would have been arguably reasonable. Enough for reasonable doubt in court.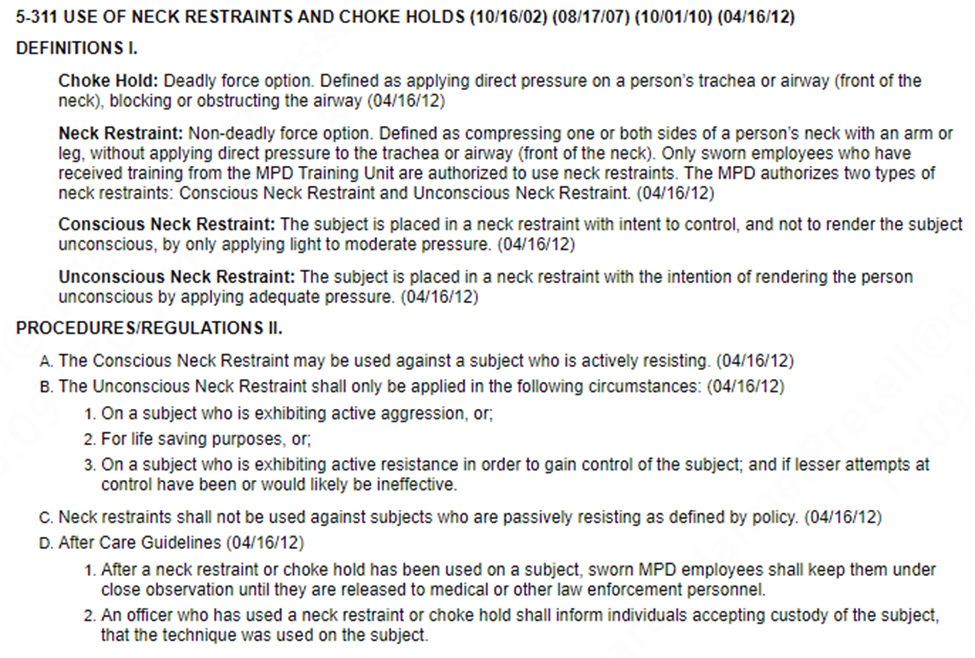
8. According to the autopsy report, Floyd had bruises and abrasions on his left shoulder and the left side of his forehead, cheek, and mouth. This is the side of his body that Floyd placed himself on the pavement when he asked to be taken to the ground. Floyd also had abrasions on his nose. Yes, people who are resisting arrest while in the prone position usually will have bruising and scrapes.
9. Balko claims that the 2014 MPD manual called for officers to roll suspects over as soon as reasonably possible. And that it did so because four years earlier, Smith died because police officers failed to do so. A few problems with this claim as well. One, that instruction is for the MRT. We have already determined that Chauvin wasn’t applying the MRT. We also established that Chauvin had a reasonable reason to wait. He was waiting for the imminent EMT that went to the wrong address. What about the slide? The slide that Balko correctly determined that only Lane saw, lists, first, that after a violent struggle, sudden cardiac arrest can occur, and then secondly, that to avoid positional asphyxia, the person should be placed in the recovery position. Again, no mention of MRT. This slide could easily be read in two ways. Especially by officers, who are not doctors. And the problem is that both ways are plausible. That once you have a sudden cardiac arrest you should put the person in a recovery position so as to avoid positional asphyxia, or what is more likely, but does not overcome that fact that it could be read the other way, that to avoid sudden cardiac arrest due to positional asphyxia, you should put the person in the recovery position. But officers don’t have the hindsight of Balko to do research on positional asphyxia such that they could overcome years of training, so what they understood and what was actually taught by the trainers is key. And again, this was taught to Lane. No evidence this was taught to Chauvin. Another fun point. We know the slides are not referring to MRT because neither the prone restrain nor the recovery position slides mention it, nor do we see any hobbles in place which are what MRT is.
10. Next, Balko shows a 2003 training video, also from the NYPD, that diagrams how positional asphyxia works. A video that was not from the Minneapolis police, and therefore irrelevant. But pretty sad, considering Eric Garner also died of positional asphyxia and Pantaleo and company got off because the focus incorrectly, just like in the Floyd case, was made on a supposed choke, instead of the much more relevant compression asphyxia they experienced. Obesity, pre-existing conditions and drugs are known to exacerbate positional or compression asphyxia.
11. Balko and Willemedia claim that TFOM did deceptive editing to falsely claim that Blackwell and Arredondo lied on the stand. This is provably false. The prosecutor asked Blackwell — who previously oversaw MPD’s training — if the technique depicted in “Exhibit 17” is an approved MPD technique. Not if it was MRT. It was. And we know it because of the slide about when to put someone in the recovery position that Lane was trained with. It clearly shows the person in the picture using the same technique. More importantly, Chauvin’s technique had been reviewed when internal affairs reviewed prior complaints of use of force where he clearly used the same technique. Chief Arradondo also lies by claiming that the technique was not taught, which is provably false, based on the slide, which is not about MRT. And when he retorts that MRT is only trained for use with a hobble, when discussing what Chauvin was doing. Which was not MRT. This is a strawman. By claiming that MRT is only used to apply a hobble, he is claiming that Chauvin was trying to do the MRT. We know that is not the case. That Lane suggested it, but that they did not do it. And the instructions for doing the MRT would not apply to the restraining position Chauvin was carrying out. In fact, we know they lied because they added the prone position to the latest iteration of their manual because it was not inly a part of MRT. And did not retroactively apply to Chauvin. Why did they lie? We can speculate: Smith required them to have training to avoid positional asphyxia, and the latest investigation by the MPCOC suggest they didn’t have proper training. By making it about improper use of the MRT, they moved the focus away from positional asphyxia. And their failure to properly train Chauvin and Thao, at the very least.
12. “We also know that of all the officers on the scene when Floyd died, only one probably saw the slide during his training: Thomas Lane. He’s the only officer who would have been a cadet when that slide was part of the MPD’s academy training.” . I quote: “That training “was originally created in 2018 for the MPD Academy” and was shown to “Cadets and Recruits . . . while they are participating in the MPD Academy.” Officer Mackenzie indicated, however, that “this presentation” has never “been included in the in-service training” provided “for the purpose of continuing education” for existing officers. As a result, Chauvin would never have seen or been trained using this slide or photograph prior to Floyd’s death.” so the slide could only show that the technique of putting the knee near the neck was not an anomaly, not that Chauvin was aware of the specific wording and instruction on the slide. W also have the image from Chauvin’s training manual that shows that Chauvin was trained on the prone restraint position using the knee to corroborate this.

What else do we know about Thomas Lane? Well, we know that he was the one officer on the scene who seemed to understand how important it is to roll a suspect into the recovery position. If anything, an argument could be made that Lane failed with his more recent training, but considering that the recent investigation by the MPCOC found there was scant evidence of proper training on positional asphyxia, I think he was innocent as well. In fact, he stated that the reason he believed it might be good to roll Floyd over was excited delirium, not positional asphyxia.
13. I quote: “The claim that “Chauvin’s knee blocked Floyd’s airway” is not the “entire narrative.” It isn’t the narrative at all. It never was. Blocking the airways isn’t the only way to asphyxiate someone. And it isn’t what killed George Floyd.” Balko is partially right here. Positional asphyxia was a factor and the knee to the neck was not what killed Floyd. So, Balko even admits what people charged Chauvin with was not what killed Floyd. But what he fails to prove is that Chauvin and the others were properly trained in Positional Asphyxia. More importantly, while a factor, it was not the only factor.
14. Balko argues that under Minnesota law, the state only needed to show that if not for Chauvin’s actions, George Floyd would not have died that day. It doesn’t matter if Floyd was more fragile or susceptible to a heart attack than most men his age. There’s a legal concept sometimes called “eggshell theory,” which states that perpetrators take their victims as they find them. It’s commonly used in tort law, but it applies to criminal law as well. If the prosecution can demonstrate that Chauvin’s use of force against Floyd was illegal, than he can be convicted. But, as Balko himself points out, they have to prove that Chauvin was doing something illegal, and as we have analyzed, there is no evidence he was. Moreover, the eggshell rule applies to innate fragilities, not self-induced fragility. Balko claims Floyd showed no signs of someone in the midst of an overdose. That an opioid overdose makes you lethargic and sluggish. That Floyd was erratic and energetic. He was standing, walking, and talking. But we know Floyd was ingesting drugs that day. He even fell asleep in the car. We also have a pretty good idea that he swallowed more pills to hide evidence. He did once before and ended in the hospital. We know Those pills would take time to take effect, more than likely around 20 minutes when orally ingested, and considering he was already on drugs, when they took effect, they would kick in with a higher level of strength. Furthermore, we know Floyd ingested two drugs, not one. Fentanyl and methamphetamine. Fentanyl and methamphetamine can affect behavior in different and sometimes opposite ways. Fentanyl can cause confusion, drowsiness, and reduced alertness, while methamphetamine can cause euphoria, hyperactivity, and increased alertness. We do not know which he put in his mouth when being arrested. Moreover, both drugs can also cause hallucinations, paranoia, and anxiety in high doses or with chronic use. The interaction of these two drugs can be unpredictable and potentially dangerous, as they may counteract or enhance each other’s effects. For example, methamphetamine may mask the respiratory depression caused by fentanyl, or fentanyl may intensify the serotonin syndrome caused by methamphetamine, leading to seizures. As Balko likes to speculate, on why Floyd claimed he couldn’t breathe, claiming it was induced by his claim of claustrophobia, which makes no sense, as Floyd was acting erratic even before there was an attempt to place him in the car, and who had been in cars and prior arrests without claustrophobia, a man who had a prior MO of acting erratic and making false claims, in the same way he did with Chauvin and company, to try to get out of arrest. If we are to assume some type of fear crisis, there is one reason readily available. Floyd knew he had ingested a bunch of drugs, and he knew he had ended in the hospital before for doing the same thing. He could plausibly have a credible fear that if he was arrested, he could die in confinement from his hasty drug consumption, unless he admitted he had just ingested more drugs to hide evidence. Maybe that is why he blurted, ‘I’m dead.’ Because the drugs might kill him.
HENNEPIN COUNTY MEDICAL EXAMINER’S OFFICE AUTOPSY REPORT
15. Balko claims that Chauvin’s defenders want it both ways. They want him to benefit from an interpretation of Floyd’s initial complaint that assumes it was the sign of a dangerous health crisis, but then exempt him from culpability for not treating it like one. That doesn’t hold up to water, except when you are an armchair analyzer looking at the events in hindsight. There is no evidence Chauvin would have known of his drug ingestion, only that he seemed to be erratic and showing signs of excited delirium and needed to be restrained. And that is what he was doing while waiting for an EMT, that, as far as he knew, was just around the corner.
16. Balko then goes into a long diatribe about the coroner’s report, the autopsy, etc., and how they ‘proved’ he did not die of an overdose. As we have discussed before, that has actually not been proven. The claim that he was a habitual drug addict and that the amount of drugs would not affect him, is unproven. Furthermore, we know he did end up in the hospital before. Add to this, that level of drugs in a resting state is a very different thing than those same drugs while in an agitated state and in a physical struggle. Nor do we know what interactions were going on between the Fentanyl and the methamphetamine, so while either drug may not have been fatal to him, we do not know that the combination couldn’t be lethal. Finally, we have Floyd with comorbidities, arteriosclerotic and hypertensive heart disease, and an enlarged heart that needed more oxygen to function, that also contributed to his risk of a sudden cardiopulmonary arrest. So, we have pre-existing comorbidities, excessive and hasty use of a combination of two dangerous drugs, and a physical struggle, all which could alone lead to cardiopulmonary arrest, but occurring together exponentially increased this risk, and then you have positional asphyxia added to this perfect storm. There is no way to know which of these, alone, or in combination, caused his death. Enough to create reasonable doubt. Finally, a forensic analyst recreated the scenario carefully measuring the positions and time and found that in his recreation no such risk of death occurred. Further accentuating, that except for those other factors, and as Chauvin himself experienced in prior use of the technique, there was no automatic risk of death. No matter how you look at it, based on the evidence, Chauvin’s use of force on Floyd leading to a death was very much an unpredictable occurrence. It was not a “departure from policy.” And Balko’s prevarications do not change that.
HENNEPIN COUNTY MEDICAL EXAMINER’S OFFICE AUTOPSY REPORT
17. Balko states that Hughes is wrong for stating “So while it is not unreasonable to think that Chauvinʼs knee was the cause of Floydʼs labored breathing, itʼs also not unreasonable to think that his labored breathing was caused by other factors—for instance, the stress of the arrest in general, the fentanyl in his system, his preexisting health conditions, or some combination of the three.” He wasn’t. I would have clarified that itʼs also not unreasonable to think that his labored breathing was caused by other factors—for instance, the stress and exertion of the arrest in general, the fentanyl and the methanfetamines in his system, his preexisting health conditions, or some combination of the three. In fat I would say that George Floyd could have definitely died of all three even without Chauvin, but that Chauvin’s actions unknowingly and more than likely than not, excacerbated things.
18. Balko claims that it’s far from clear that the fentanyl levels in Floyd’s system were as toxic as Chauvin’s defenders claim. For this he points to the prosecutor’s expert witness, toxicologist Daniel Isenschmid who testified that Floyd’s fentanyl levels were lower than the average levels of people charged with driving while high on the drugs — none of whom died of an overdose. But, there is a key difference. None of the cases mentioned showed that they were taking methamphetamine and opioids and involved in a high exertion activity at the time of death, resisting arrest. Balko also claims that the prosecution witness stated that Floyd’s opioid levels were about 50 percent lower than the average found in people who did die from an overdose. That is false. What the witness, Mr. Isenschmid stated was that of 19,185 cases where people died of unreported causes, could be gunshot, natural death, whatever, samples of the peripheral blood showed a mean of 16.8 ng of fentanyl and a median of 10 ng. The average is 16.8 ng. 50% less would be 8.4 ng. Moreover, we do not know what percent were from overdoses. The fact remains that Floyd’s 11 ng was higher than the median of 10 ng and over 50% of the people who died in this report had less fentanyl than him. And what other drugs and synergies, or lack of them is not in evidence either.
Reminder. George Floyd had 11 ng of fentanyl and 19 ng of methamphetamine and 2.9 ng of delta-9 THC in the blood and also 86 ng of free morphine in the urine. Free morphine is the active form of the drug. Finding it in autopsy urine suggests use relatively close to death. Morphine, especially free morphine, clears from the blood faster than from urine. It’s not unusual for it to be undetectable in blood from an autopsy, even if it was active at the time of death. Add caffeine as he testd psitive for that as well. Key point, none of these analyses talk about the synergistic effect they might have with each other, let alone the physical exertion of resisting arrest, and the preexisting medical conditions. Only the preexistent medical conditions would be relevant to the eggshell rule, if a felony was proven to have been commited. Floyd chose to take those drugs, he chose to take them together, and he chose to resist arrest. Those actions and how they interacted with each other and the preexisting medical conditions are not covered by the eggshell rule. We already addressed fentanyl and methamphetamines, but what about the others?
The combination of THC (found in cannabis) and methamphetamines (stimulants) can lead to unpredictable effects. THC may enhance the psychoactive properties of methamphetamines, potentially increasing anxiety, paranoia, and cardiovascular strain. THC and morphine both have analgesic properties. Combining them could potentially enhance pain relief, but it may also increase sedation and respiratory depression. Researchers suggest that combining THC and caffeine may have significant effects due to the interaction of the adenosine and cannabinoid systems. These substances act differently in the body, and their combined effects are not fully understood. Both Fentanyl and morphine are potent opioids. Combining them can significantly increase the risk of respiratory depression, sedation, and overdose. Fentanyl and caffeine have contrasting effects. Fentanyl depresses the central nervous system, while caffeine is a stimulant. Combining them may lead to unpredictable interactions, affecting alertness and cardiovascular function. Methamphetamines and morphine have opposing effects. Methamphetamines stimulate the central nervous system, while morphine depresses it. Combining them can strain the cardiovascular system and increase the risk of adverse effects. The combination of methamphetamines and caffeine can lead to increased stimulation, anxiety, and cardiovascular strain. Caffeine and methamphetamines are both stimulants. They increase alertness, elevate mood, and suppress feelings of fatigue. When combined, they can make a person appear awake, energetic, and less sleepy. However, the simultaneous use of these stimulants and depressants (phentanyl and morphine) can lead to a paradoxical state. While the person may not appear sleepy, they might exhibit signs of confusion and anxiety. The central nervous system experiences conflicting signals: the stimulants push for increased activity, while the depressants slow down brain function. This can result in a state of mental disarray. A masking effect occurs because the stimulants partially counteract the sedative effects of the depressants. As a result, the person may not exhibit typical signs of drowsiness or sedation. Observers might perceive the person as functioning normally due to the stimulant’s influence. Despite appearing alert, the individual’s body systems are still affected by the depressants. Respiratory depression (shallow breathing) and cardiac arrest remain significant risks. The heart may struggle to maintain a balance between stimulation (from the stimulants) and depression (from the opioids). This delicate balance can suddenly tip toward life-threatening complications. And that is before adding preexisting conditions and high exertion. What the prosecutors did was individually rule out each drug as the cause of death, but never evaluated them together for synergistic effects, nor the effects along with exertion, Methamphetamines (uppers) and caffeine (also an upper) can significantly increase heart rate, blood pressure, and overall stress on the cardiovascular system. Wrestling (resisiting arrest) is physically demanding, and the combination of these stimulants could lead to excessive strain on the heart. Morphine and fentanyl (both opioids) are depressants. They slow down the central nervous system, including respiratory function. Wrestling requires physical exertion and increased oxygen demand. Combining opioids with intense physical activity can suppress breathing and oxygen intake. The simultaneous use of uppers and downers creates a dangerous seesaw effect on the body. The heart may struggle to maintain a balance between stimulation and depression, potentially leading to cardiopulmonary arrest (heart and lung failure). Even a healthy person would be at risk of sudden cardiopulmonary arrest, And Floyd had just healed from Covid, had an enlarged heart and an artery with 75% blockage. Can you start visualizing the biologic roller coaster that Floyd was putting his system through?
Balko then claims that the witness stated that much of the fentanyl found in Floyd’s blood was norfentanyl, a byproduct the body creates after metabolizing the drug. This is actually misleading. Floyd actually had 11ng of fentanyl and 5 ng of norfentanyl. So the majority was the active fentanyl, which was above the median given for the fatality cases. Balko then states that overdoses generally occur shortly after ingestion, well before metabolization. True. But as was stated in the video, presence of norfentanyl was seen in the majority of death cases and the ratio becomes irrelevant if Floyd ingested new pills. Which there is evidence he did. You can hear Isenschmid’s testimony for yourself here. And notice what is missing and what Balko failed to note or just msrepresented.
19. Balko, and the prosecution, relied heavily on Dr. Tobin’s absolutist claims. Tobin made statements that those positions would absolutely kill anyone who was in the same positions. Made a lot of absolute claims and everyone believed him because of his stellar credentials. But I always suspected he was a zealot by the fact that he never checked the autopsy, nor the body cams, to factor it in to his analysis. He just went ahead and claimed that it absolutely was the position he was and that anyone would have died. Only Bruce Champagne, a Forensic Analyst, proved that wasn’t true. For any scientific claim to be valid, no matter how wonderful and complex it sounds, it has to be replicable. Champagne and company should have had to stop the test because he was suffering like Tobin claimed he would. And he didn’t. Furthermore, Tobin made exaggerated claims of Chauvin’s weight. One, his weight was distributed over 2 knees, not one, and his other foot was also on the ground. His weight is 140lbs. Even with full gear we are looking at 170lbs. But he wasn’t wearing full gear. His undervest, for his size and weight would only have been 5 to 7 pounds. But lets stick with 170 lbs. Tobin claimed half Chauvin’s weight was on Floyd.. That is only 85lbs. I would argue three points of contact would distribute the weight to three points so closer to 57 lbs. focusing on one point? Increase it to 60 lbs. So you are looking at roughly 60 lbs in the neck and shoulders. 40 lbs on the other knee in the mid back mid back. Not a lethal amount of weight, under normal circumstances. And this was proven by replicating the positions. It was the combo of the drugs (meth and fentanyl combined), the physical altercation, preexisting conditions and the positional asphyxia, along with medics going to the wrong address and not performing CPR until four minutes after they arrived that killed Floyd. That whole combination, a perfect storm, could not have been predicted by one cop. Now, collectively, all three officers may have caused positional asphyxia, haven’t seen anyone test that. But again, where was the training to ensure multiple cops weren’t creating a situation collectively that their individual action might not create.
AN EXPERIMENT: ROLE PLAYING DEREK CHAUVIN AND GEORGE FLOYD
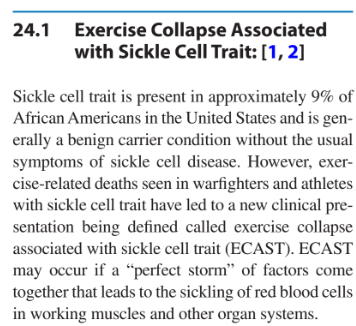
20. Balko claims that George Floyd’s sickle cell anemia couldn’t have played a role and that ‘there’s a dubious theory that black people who carry one of the two genes for sickle cell anemia are especially prone to die when exposed to the sorts of stresses that accompany a struggle with police.’ Note, the citation he provides is from an anti-racist initiative after George Floyd, and not an actual study. The statement mentions that, as reported by The New York Times, in two-thirds of the cases where sickle cell trait was incorrectly misinterpreted as the cause of death, the decedents had been forcefully restrained, beaten, pepper-sprayed, and/or shocked with stun guns. WHat the statement fails to mention is that even in those circumstances where that stressful event occured, the sickle cell trait could have been a major factor in the death, The sudden death of people with sickle cell anemia who are exercising is well documented and not a ‘dubious theory.’ Some people may abuse the diagnosis, but it is still very real. Look at 2021, Summit on Exercise Collapse Associated with Sickle Cell Trait: Finding the “Way Ahead”. Just look at 2023 Cardiac Emergency in the Athlete, where it states: Underlying cardiac abnormalities that can predispose some athletes to sudden cardiac arrest include cardiomyopathies, coronary artery anomalies, and channelopathies, as well as genetic disorders such as sickle cell trait, and Marfan syndrome. Floyd had three of them, cardiomyopathies, coronary artery anomalies and the sickle cell trait. Is Balko saying that a person who has a cardiac arrest while running with sicke cell anemia has died solely because of the running per se? Further reading from 2023, Determinants of ventricular arrhythmias in sickle cell anemia: toward better prevention of sudden cardiac death, and 2024, Hematologic and Endocrine Conditions: Exercise Collapse-Associated with Sickle Cell Trait, Exertional Rhabdomyolysis, Hyperglycemia, and Hypoglycemia,
21. “The Flattening’ This will be a separate blog as there is much to cover that is not directly related to Derek Chauvin and George Floyd. This will be a placemarker for a link to that future blog.

Leave a comment